This disease causes a child to have an abnormally tiny lower jaw when they are born. The condition can create problems with feeding and breathing. Obstructive sleep apnea (OSA) may be a symptom of breathing difficulties, which can have a negative impact on energy and quality of life. OSA is more common in people with micrognathia than it is in the general population. Children with micrognathia have a much higher risk of severe OSA than the general population.
What Is Micrognathia?
When a kid is born with a smaller lower jaw than is typical, the condition is known as micrognathia1. Feeding and breathing are two of the more common symptoms. One of the most common causes of sleep deprivation and exhaustion is obstructive snoring (OSA). The prevalence of OSA is significantly higher in people with micrognathia than it is in the general population. Most children with micrognathia have severe OSA, compared to just 2% of the general population who suffer from the condition.
You are reading: What Is The Most Common Cause Of Obstructive Sleep Apnea?
Aside from difficulty eating or breathing, pauses in breathing (which may be an indication of sleep apnea), hearing issues, and trouble sleeping may all be signs of micrognathia. Children with micrognathia may struggle to eat, and 88% of them have snoring problems, according to the American Academy of Pediatrics. People with micrognathia are also more likely to suffer from gastroesophageal reflux.
At adolescence, it is possible that the condition of micrognathia will go away on its own without treatment. Micrognathia can create developmental issues when the disorder is still present. Obstructive sleep apnea can develop as a result of the infant’s inability to adequately feed, grow their teeth, or breathe during the night.
Micrognathia and Obstructive Sleep Apnea
Sleep apnea, also known as obstructed breathing while sleeping (OSA), increases a person’s risk of cardiovascular, neurobehavioral, and metabolic problems. Snoring and choking are common symptoms of Obstructive Sleep Apnea (OSA). A person’s sleep quality deteriorates even if they don’t wake up during an apneic episode, leading to signs of sleep deprivation such as fatigue, mood swings, and lack of concentration.
Pediatric OSA can lead to headaches, hyperactivity, and learning and behavioral issues due to sleep deprivation. As a result, the growth of children with OSA may be negatively impacted by low blood oxygen saturation levels.
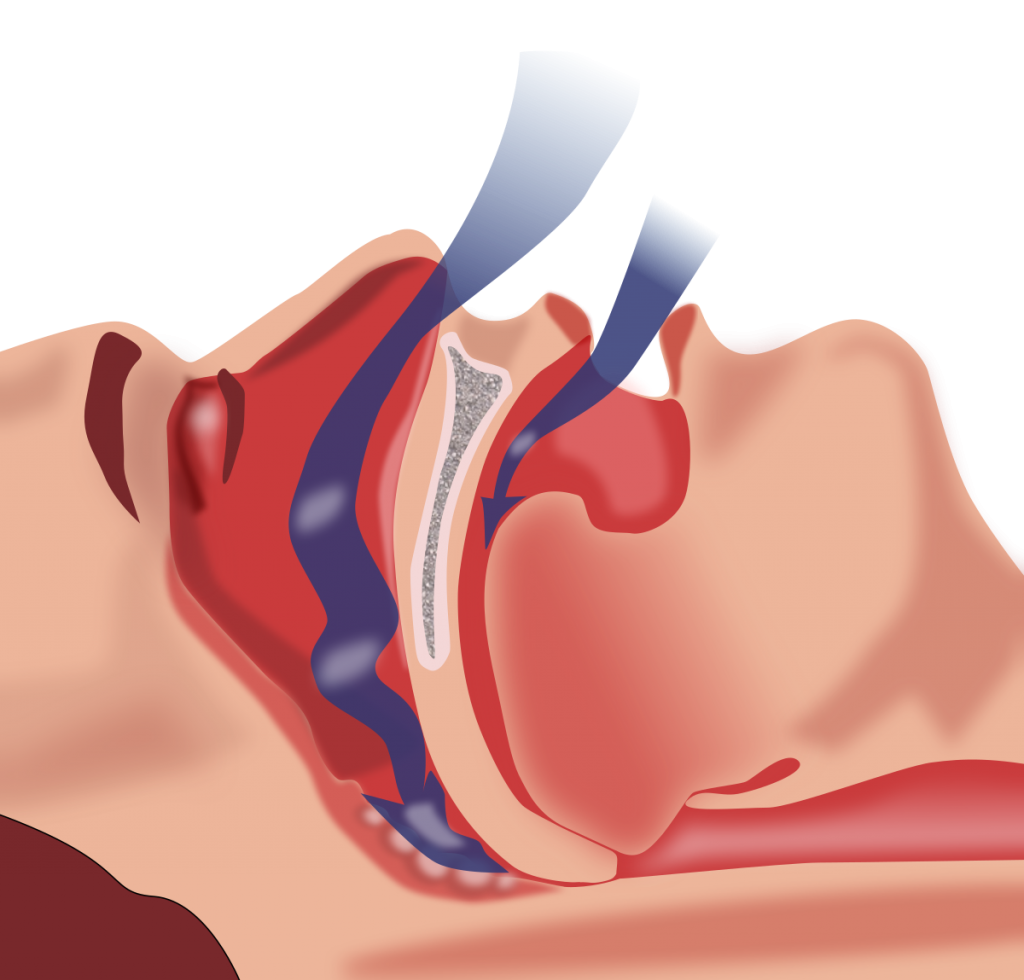
Overweight or enlarged tonsils might lead to the development of obstructive snoring (OSA). Micrognathia is a condition in which the lower jaw is abnormally tiny, causing the tongue to hang back and obstruct the airway.
Read more : Can Your Thyroid Cause Sleep Problems? What You Can Do?
The number of apneic episodes a person has during the course of a night is used to assess the severity of OSA. Additionally, children with micrognathia are more prone to suffer from severe forms of obstructive sleep apnea (OSA). In comparison to the average kid, a child with micrognathia experiences roughly sevenfold more apneic episodes each hour.
What Causes Micrognathia?
Most micrognathia sufferers are born with the condition. Genetic mutations or inherited disorders that create facial deformities such as small lower jaws may be responsible for micrognathia.
- Achondrogenesis
- An abnormality of the lips or palate
- Syndrome of the crimson cat
- Fetal alcohol spectrum disorder
- Syndrome of Hallermann-Streiff type
- Syndrome of the Goldenhar
- Needless to say, Melnick suffers from Melnick syndrome.
- Marfan’s disease
- The Nagar condition
- Sequenced by Pierre Robin
- Progeria
- Syndrome of Russell-Silver
- “Seckel’s disease.”
- Irritable Bowel Syndrome (IBS)
- the syndrome of Treacher-Collins
- The condition is known as Trisomy
- Trisomy is the most common form of the disorder.
- Trisomy,
- The XO disorder
Most micrognathia-causing genetic disorders are extremely uncommon. Pierre Robin sequence, for example, affects 1 in every 8,500 to 14,000 newborns11, while trisomy affects 1 in every 16,000 newborns12.
How Is Micrognathia Diagnosed?
It is fairly unusual to find out if a child has micrognathia during their first year of life, if not earlier. The first trimester of pregnancy is the best time to check for micrognathia because it is when the condition is most easily diagnosed with ultrasonography.
Pediatricians are the best people to go to if you find that your child’s jaw is too small or if they are having difficulty eating or breathing. The misalignment of your child’s teeth may continue to cause difficulties in eating and speaking as they grow older. The symptoms of sleep apnea, such as trouble sleeping and hyperactivity or exhaustion during the day, maybe present in your child. You may hear them choking, gasping, or making loud snoring noises while they are sleeping.

Starting with an examination of your child’s lower jaw and the position of their tongue and lower jaw, your doctor will be able to determine if your child has micrognathia. If your child’s lower jaw and the rest of their skull aren’t properly aligned, an X-ray or CT scan may be necessary. It’s possible that your doctor will also inquire about when you first noticed how large your child’s jaw was and whether they have problems eating or breathing.
A polysomnogram, or nightly sleep study, may be ordered by your doctor if your child shows indicators of sleep apnea. As your child sleeps, doctors monitor their breathing, brainwaves, blood oxygen levels, and heart rate in a lab.
Treatment Options for Micrognathia
When it comes to treating micrognathia, there are a variety of options. As the child’s jaw develops, it’s possible that micrognathia will go away on its own. As a result, some parents may delay treatment in order to see if the issue may be resolved without the need for intervention.
Read more : How To Determine Poor Quality Sleep? Professional’s Guide
Severe conditions may necessitate more immediate treatment, including problems with nutrition and breathing. Different feeding positions may be recommended by a doctor to help a newborn with feeding difficulties. CPAP therapy or oral surgery can be beneficial in treating respiratory issues.
CPAP Therapy
For the symptoms of obstructive sleep apnea, your doctor may suggest sleeping in a modified position or prescribing CPAP therapy. CPAP machines provide compressed air into the mouth through a face mask attached to the machine, keeping the airways open for the user.
CPAP therapy dramatically improved sleep apnea symptoms in adolescents and young adults with micrognathia, according to research. It’s not recommended to utilize CPAP therapy in cases when the airway is restricted by swollen tissues because it’s meant to be a temporary solution. CPAP therapy may show the need for surgical intervention in certain patients.

Mandibular Distraction Surgery
Oral surgery may be recommended by doctors based on the severity of a person’s micrognathia and its etiology. Treatment options for crooked teeth include braces or surgery. As a result of tongue-tip adhesion and mandibular distraction osteogenesis (MDO), the lower jaw can be gradually extended by removing or adding bone.
These operations are often successful, although recovery takes time. Feeding and respiratory issues should be resolved by six months to one and a half years. After surgery, the symptoms of sleep apnea should be much reduced. There are fewer apneic episodes and improved or restored blood oxygen saturation values.
Among people with micrognathia, 80% had their sleep apnea corrected with MDO surgery, while the rest had significant improvement. Similar findings were found in a trial of infants, with MDO surgery either considerably reducing or eradicating sleep apnea symptoms. It’s also been proven that reducing or eliminating the symptoms of sleep apnea can be accomplished by strengthening the tongue-lip bond.
Micrognathia has the best prognosis if diagnosed early. As soon as a doctor is able to identify the problem, he or she will be better equipped to select the best course of action.
Vote for this post!
Source: https://bestpillowsleepers.com
Category: Sleep Advisors









