It’s estimated that as many as 25 million Americans suffer from the sleep-related breathing disease known as obstructed airway syndrome (OSAS). They regularly wake up coughing or gasping for air because of OSA2. Sleep disorders like narcolepsy can lead to increased daytime tiredness despite the fact that these episodes typically last no more than 30 seconds at the most
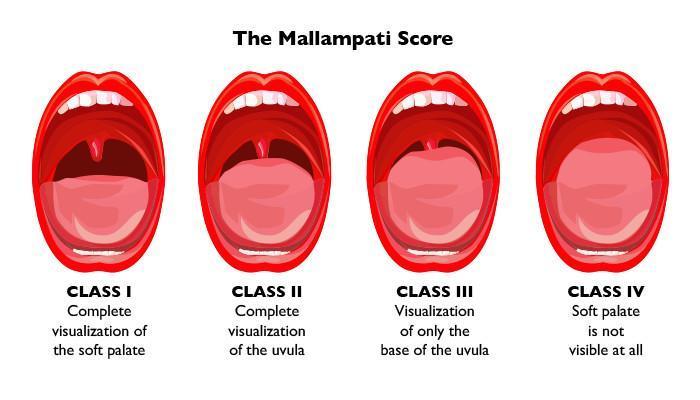
The Mallampati score has been used by certain doctors and researchers to assess the risk of OSA in patients. Using a 1 to 4 scale, the Mallampati score estimates how difficult it will be to intubate a patient’s tongue and esophageal airway. For children, the Mallampati score may be a reliable indicator of OSA and may help prioritize patients for a sleep study and/or referral to sleep medicine. Other research has produced ambiguous results.
What Is Obstructive Sleep Apnea?
At some point throughout the course of your slumber, you may experience gasping or choking episodes, which are indicative of a sleep problem called apnea. There is a physical obstruction in the airways of people with OSA, which makes it difficult for them to breathe and causes their symptoms. An enlarged tongue or tonsils, a retracted lower jaw, or a thick neck circumference are all possible causes of this obstruction6. Central sleep apnea (CSA), on the other hand, happens when the brain and muscles that enable breathing are interrupted.
OSA affects 2% to 9% of individuals, with the majority of cases going undiagnosed. In many cases, the AHI8 is used to assess OSA severity, however this method has certain drawbacks. “Apnea” refers to a total cessation of breathing, whereas “hypopnea” refers to a partial collapse of the airway but not a complete cessation of breathing. Apnea and hypopnea episodes per hour of sleep are classified into three general categories by the AHI: mild, moderate, and severe.
- Mild: 5 to 15 a day or more.
- Slow: 15 to 30 per hour
- Over 30 per hour is considered severe.
When assessing the severity of OSA, doctors will look at additional factors. Obesity is a significant risk factor for OSA, and BMI is frequently used to assess this risk. Obesity is defined as a body mass index (BMI) of 30 or higher. Snoring and excessive daytime sleepiness are also taken into consideration by doctors. Although polysomnography (sleep study) is the gold standard for OSA diagnosis, severity classification, and treatment monitoring, it has several drawbacks such as high cost and difficulty in accessibility. As a result, the AHI has long been regarded as the key indicator of OSA severity.
What is the Mallampati Score?
Patients with an oropharynx that is difficult to intubate can be identified using the Mallampati score, which was first introduced in 1985. Based on a 1 to 4 scale10, this score has the following criteria:
Tongue, uvula and soft palate are all clearly apparent.
It’s possible to see the hard and soft palates as well as the upper tonsils and uvula.
Uvula is partially hidden, but the hard and soft palates are clearly evident.
The patient’s mouth is open and their head is in a neutral position during this assessment. Since OSA has been linked to a higher risk of intubation, it is common for individuals with a Mallampati score of 3 or 4 to be diagnosed with the illness.
Researchers, on the other hand, have observed varying degrees of success in predicting OSA using Mallampati scoring. Children’s tonsil size and Mallampati score were found to be strongly linked in a single study. For children with OSA and those without it, this study found conclusive results.
This method of measuring OSA has been called into question by other studies. According to another study, the Mallampati scale and AHI have a strong association, however there is very little variation in AHI amongst the different Mallampati classes. The combination of BMI, gender, and age was a better predictor of AHI in this research of adult patients than the Mallampati scoring.
Although it can be used before polysomnography sleep studies, the Mallampati score has several limitations as a diagnostic evaluation. The odds of a patient getting OSA more than doubled for every one-point increase on the Mallampati scale. For physical examinations, a Mallampati assessment can provide important information, but the study authors admit that it is less effective for individuals with moderate OSA symptoms.
Note that the AHI assessment has its critics as well. Some studies have criticized the AHI for focusing simply on the number of apneas and hypopneas per hour of sleep without taking the duration of each episode into consideration, as longer episodes pose a greater danger to the patient’s general health. Because of additional factors such as age and daytime symptoms, the AHI may not be totally accurate in determining how severe a patient’s OSA symptoms are.
Obstructive sleep apnea (OSA) symptoms
Pediatric sleep apnea (OSA) can cause the following symptoms;
- Unusual patterns of breathing when sleeping
- Restlessness or frequent wakings
- Constantly haunting dreams
- Enuresis
- A hard time getting out of bed.
- drowsiness during the day
- Hyperactivity/behavior problems
- Hyperactivity/behavior problems
- Hyperactivity/behavior problems
OSA Diagnosis
Hyperactivity/behavior problems
Behavior and/or hyperactivity issues
If you have any reason to believe your child is suffering from sleep apnea, make an appointment with Airway and Sleep Group now. We’re ready to assist you at any time!
Mallampati Score to Help Predict Obstructive Sleep Apnea
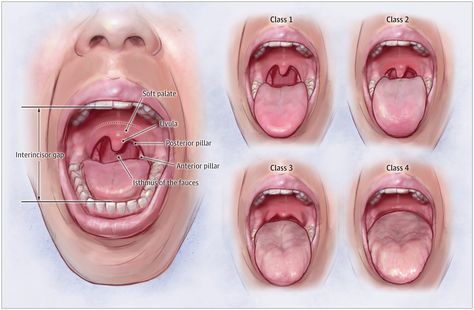
Dr. Hirschinger in Beverly Hills will examine your mouth to see if you have obstructive sleep apnea during your initial examination. He’s checking to see if your airway is open, among other things. Anesthesiologists also use this method to check your airway prior to any procedure that would necessitate intubation in order to add or remove fluids from your stomach. Certain structures in your mouth can restrict or constrict your airway when you open it. This is what they look like:
Due of its lack of bone, the soft palate is appropriately termed. Because it contains bone, the region immediately before the soft palate is referred to as the hard palate. During swallowing, the soft palate serves to shut the nasal passages.
When it comes to taste, the tongue is the most important organ.
These lymphoid tissues are known as the tonsils, and they can swell if infected, which is called tonsilitis. In order to breathe through the mouth, the airway becomes smaller as they enlarge.
The little patch of tissue that hangs from the soft palate’s edge is known as the uvula, which means “little grape” in Latin.

Mallampati I
A Mallampati I score is given to anyone who can clearly make out their uvula while their tongue is extended.
Mallampati II
The Mallampati II score is given if the tongue partially covers the uvula while the airway is largely unobstructed.
Mallampati III
We score Mallampati III if the tongue covers most but not all of the uvula when we look inside with the tongue extended.
Mallampati IV
Mallampati IV is given if the tongue extends all the way down and completely hides the uvula; this indicates that the airway is extremely restricted.
What do you think?
![Top Rated CPAP Machine Buyer’s Guide [current_date format=’m/Y’]](https://bestpillowsleepers.com/wp-content/uploads/2023/03/best-cpap-machine-img_6405d72310053-400x300.jpg)
![The 11 Best Cooling Weighted Blankets [current_date format=’m/Y’]](https://bestpillowsleepers.com/wp-content/uploads/2023/01/best-cooling-weighted-blankets-img_63d4ff15c615d-400x300.jpg)
![Ultimate Guide to Choosing a Best Cooling Mattress Pads [current_date format=’m/Y’]](https://bestpillowsleepers.com/wp-content/uploads/2023/01/best-cooling-mattress-pads-img_63c403115126b-400x300.jpg)
![Ultimate Guide to Choosing a Best Cooling Mattress [current_date format=’m/Y’]](https://bestpillowsleepers.com/wp-content/uploads/2023/01/ultimate-guide-to-choosing-a-best-cooling-mattress-img_63bcdba870d77-400x300.jpg)
![Ultimate Guide to Choosing a Best Cooling Comforters [current_date format=’m/Y’]](https://bestpillowsleepers.com/wp-content/uploads/2023/01/ultimate-guide-to-choosing-a-best-cooling-comforters-img_63bba2f5cd3ce-400x300.jpg)